Living rules to prevent COVID-19
| PREVENTION METHOD | THE REASON |
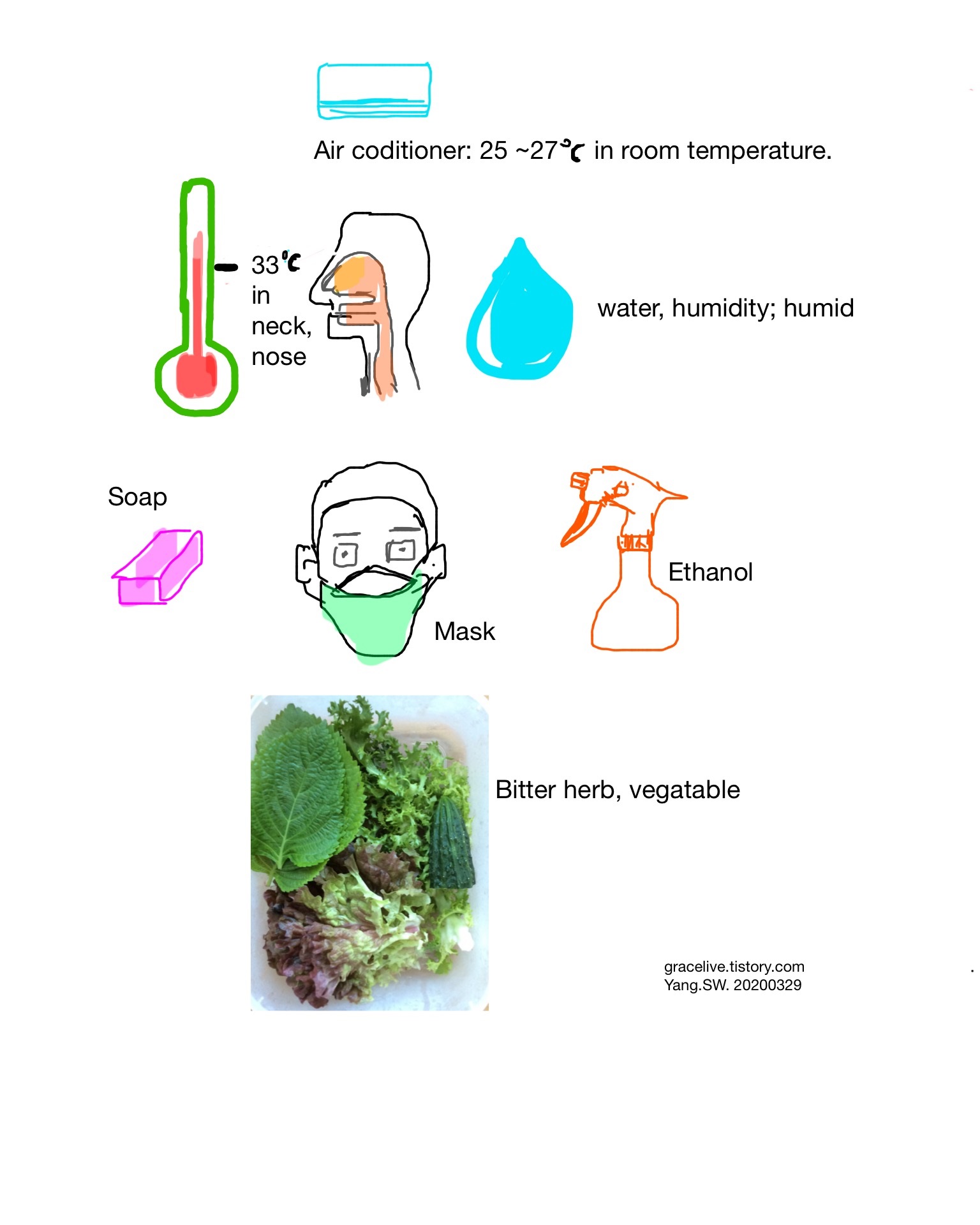
| Temperature |
The optimal temperature for coronaviral proliferation is 33 °C. This temperature is the normal temperature in the upper respiratory tract. Hence, to keep the temperature in the upper airway more than 33°C is recommended. |
| Humidity | In cold and dry state, the viability of coronavirus is high. |
| Facial mask | Facial mask filters viral droplets and makes human upper airway keep warm and humid. |
| Air conditioner, Room temperature. |
Room temperature is 20 ~ 22 °C. In this temperature zone, the temperature of the upper airway is 33 °C. To keep the upper airway in more than 33°C, the room temperature should be more than 23°C As my personal experience considering both temperature and humidity, the adequate temperature of air-conditioner may range from 25 to 27°C. |
| Soap, Disinfectant | |
| Ethanol, Disinfectant | Ethanol plays a role in breaking enevelope of coronavirus. |
| Bitter herbs, Food | Bitter herbs help our immunity boost. |
| Mediterranean diet | Meditteranean diet helps our immunity boost. |
For detailed explanation, refer to category "2019-nCoV, COVID-19" within this blog.